Discovery
Dr. Klaus Patau, 1960
German-American Born 1908, Died 1975 Geneticist University of Wisconsin
Patau syndrome was first identified as a distinct chromosomal syndrome in 1960 by Dr. Klaus Patau, a German-born American geneticist, with his team at the University of Wisconsin. Patau published his landmark paper "Multiple congenital anomaly caused by an extra autosome" in The Lancet.
Although the clinical symptoms of Patau syndrome had been observed as early as 1657 by the Danish doctor Thomas Bartholin, it was Patau and his team who first provided a genetic explanation. This disorder has borne his name ever since.
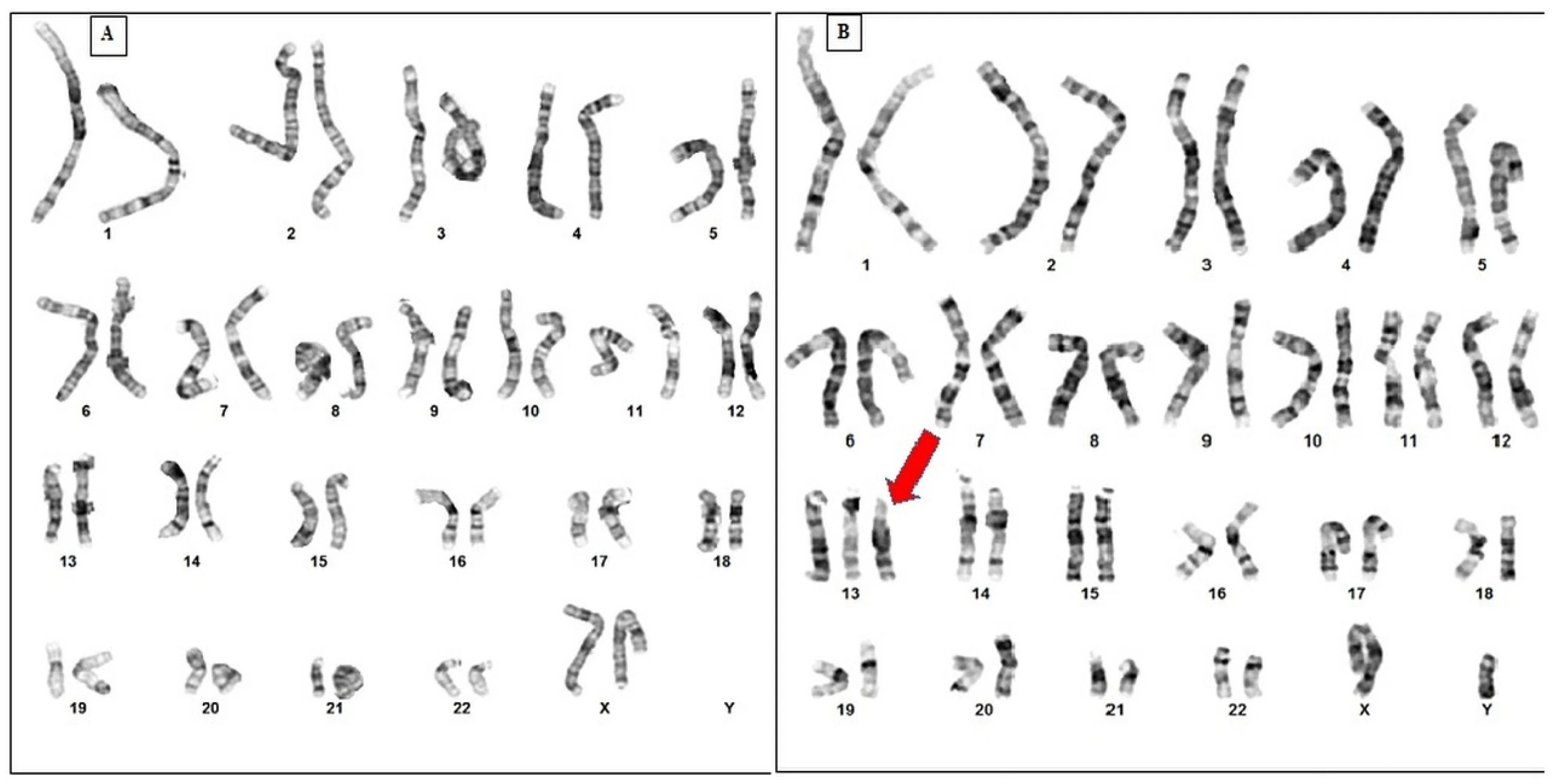
In the study, Patau's team identified 47 chromosomes in a patient's bone marrow cells, instead of the normal 46. There was an extra copy of chromosome 13, forming a trisomy, which caused the distinct symptoms of the genetic disorder.
Signs & Symptoms
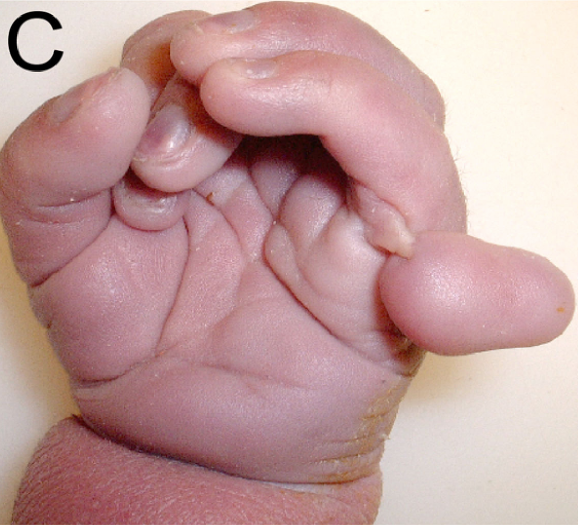
Excess genetic material carried by the extra chromosome 13 disrupts normal development, leading to extensive physical and intellectual malfunctions. However, symptoms may vary in severity depending on whether all or only some cells carry the extra chromosome. The situation where only some of the somatic cells carry the extra chromosome is known as mosaic trisomy 13.
Common symptoms of Patau syndrome include: (Most common symptoms are bolded)

Chromosome Affected & Inheritance
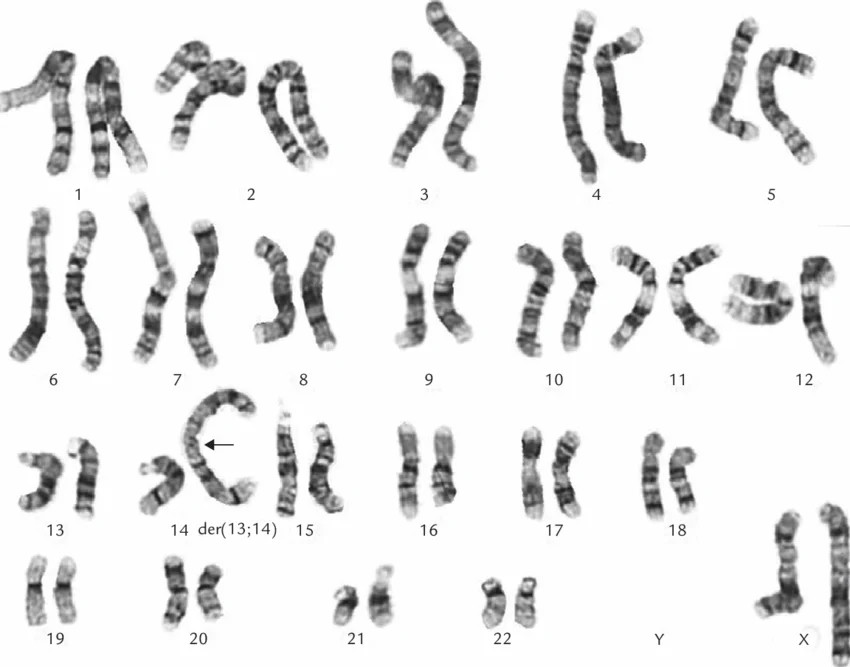
Partial (Translocation) Trisomy 13: ~15%, part of chromosome 13 bonds to another chromosome nearby, which doesn't change the total number of chromosomes but may still cause symptoms
Mosaic Trisomy 13: ~5%, only some cells have the extra chromosome, results in milder symptoms
Mechanism of Inheritance
MOST cases are not inherited. Full trisomy 13 is caused by random errors during sperm or egg formation, mainly nondisjunction. When homologous chromosome pairs or sister chromatids of chromosome 13 fail to separate properly during meiosis, one gamete ends up with two copies of chromosome 13, and another with none. If the gamete with the extra chromosome 13 is fertilized, every cell of the resulting embryo will carry the extra chromosome.
In some rare cases, nondisjunction during mitosis after the embryo has started developing can lead to mosaic trisomy 13, where only some cells possess the extra chromosome 13.
The exception is translocation trisomy 13, which can be potentially passed down from a parent who carries a balanced rearrangement between chromosome 13 and another chromosome, which shows no symptoms. During the formation of his/her gametes, the uneven separation of chromosomes may disrupt the balance and result in an affected child. However, not all translocation trisomy 13 are inherited from parents, as the translocation may also occur naturally.
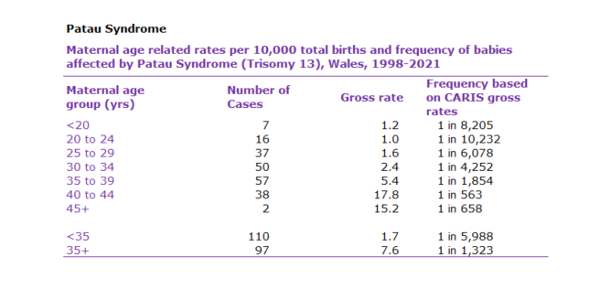
Other than all those random factors, it is known that the mother's age has a strong correlation with the risk of nondisjunction errors and thus Patau syndrome. The risk will rise substantially if the mother is more than 35 years old.
Treatment Options
There is no cure for Patau syndrome. Treatment is considered on a case-to-case basis and focuses on managing symptoms and providing comfort to terminal individuals.
Cardiac Surgery
In some cases, heart defects may be surgically repaired to offer prolonged survival.
Cleft Lip or Palate Repair
Surgical repair of a cleft lip or palate can improve feeding and speech ability.
Other Surgeries
According to each case, other surgeries may be conducted to correct a certain physical deficit.
Seizure Management
Medications can be used to manage epileptic seizures, which affect 25–50% of surviving patients.
Respiratory and Nutritional Support
A ventilator or feeding tube may be used to help with breathing or eating difficulties.
Rehabilitation Therapy
Physical, occupational, and speech therapy can help surviving patients approach their maximum development potential.
Pain Management and Palliative Care
For many families, ensuring the comfort of the terminal patient and maintaining dignity is chosen over aggressive treatment options.
Alternative & Complementary Approaches
While no alternative medicine can treat the chromosomal abnormality itself, the following are sometimes used to support quality of life in long-surviving patients:
Music and Sensory therapy: Provide emotional stimulation and help improve responses and calm in child with severe neurological conditions.
Massage therapy: Reduce muscle tension and improve the comfort of the child.
Controversy: Is Patau Syndrome Truly "Lethal"?
For decades, Patau syndrome was labeled a "lethal" disorder, and most hospitals offered only palliative care. However, new pieces of evidence show that aggressive intervention, such as cardiac surgery, mechanical ventilation, and intensive care, can extend survival significantly. A Japanese study found median survival could be extended to 733 days with intensive management. However, Is prolonging life also prolonging suffering?
This controversy heavily lands on the intersection of ethics and economics. As clinical outcomes demonstrate that Patau syndrome is not strictly "lethal" in a medical sense, it becomes difficult to debate whether the goal of medicine is to prolong life to its full limit or to optimize its quality and reduce suffering. This forces us to question the extent parents should be allowed to intervene in the treatment plans of their children. Ultimately, even though aggressive intervention may offer a slight benefit for survival, the prohibitive financial costs and the potential for extended physical and mental distress are usually factors that limit the options families are willing to take.
In the research paper, Wilkinson and his colleagues argue that well-informed parents should be given a stronger voice in these decisions than has traditionally been the case. They suggest that the historical practice of withholding aggressive care without meaningful parental input may itself be ethically problematic. In simple words, the controversy itself is not merely about the medical statistics, but about who has the right to decide and on what basis.
Statistics Related to Patau Syndrome
References
- Bhatt, V., & Singh, S. (2024). Chromosomal abnormalities and clinical manifestations of Trisomy 13. Journal of Genetic Medicine, 12(3), 145–152.
- Cleveland Clinic. (2025, December 8). Trisomy 13 (Patau syndrome): Symptoms, causes, and outlook. https://my.clevelandclinic.org/health/diseases/24647-trisomy-13-patau-syndrome
- Mana'a, M., Ananzeh, M., Murad, M., & Aqel, M. (2025). Multidisciplinary intervention for Patau syndrome patient with long-term survival: A case report of single institution-based detailed clinical management. PMC — National Library of Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC12063923/
- MedlinePlus Genetics. (n.d.). Trisomy 13. U.S. National Library of Medicine. https://medlineplus.gov/genetics/condition/trisomy-13/
- Nelson, K. E. (2023). Ethical dilemmas in the management of trisomy 13 and 18: A re-evaluation of 'lethal' labels. American Journal of Bioethics, 23(1), 12–24.
- Patau, K., Smith, D. W., Therman, E., Inhorn, S. L., & Wagner, H. P. (1960). Multiple congenital anomaly caused by an extra autosome. The Lancet, 275(7127), 749–751.
- Schaffer, A., & Bhimji, S. S. (2023, June 26). Patau syndrome. StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK538347/
- Wilkinson, D., Thiele, P., Watkins, A., & De Crespigny, L. (2018). Management options and parental voice in the treatment of trisomy 13 and 18. Journal of Perinatology, 38(11), 1488–1495. https://doi.org/10.1038/s41372-018-0151-6